标签:
http://www.intechopen.com/books/liver-tumors-epidemiology-diagnosis-prevention-and-treatment/epidemiology-and-risk-factors
世界卫生组织数据报告:
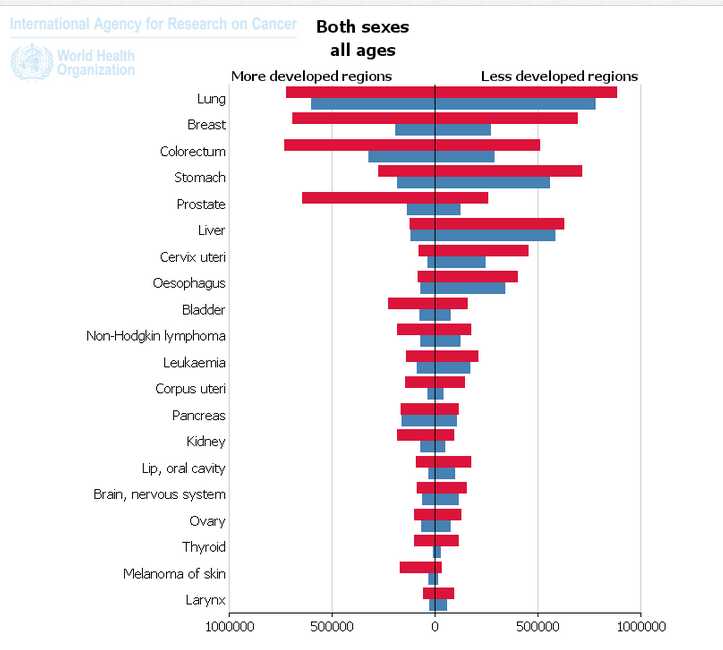
相同性别,和年龄前提
发达国家和发展中国家各种癌症对对比,包括感染率和死亡率
发达国家前列腺感染率高,但死亡率低,因为良好治疗条件

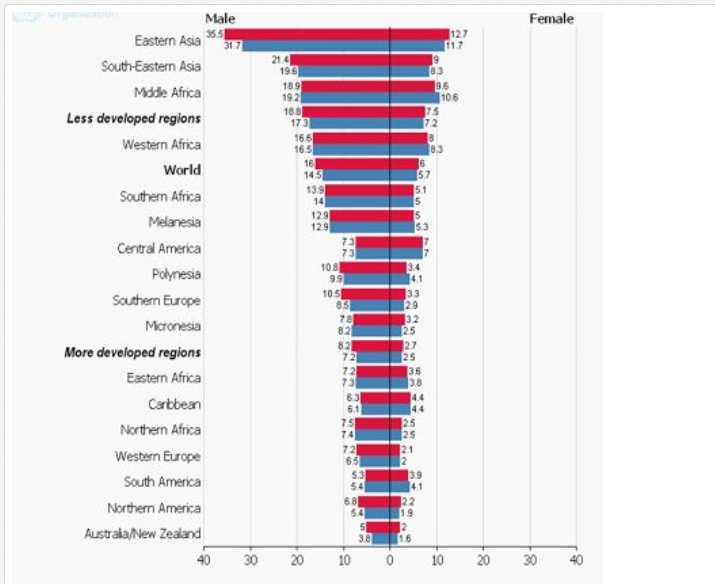
全球HCC感染率和死亡率----男女对比
男性远远高于女性
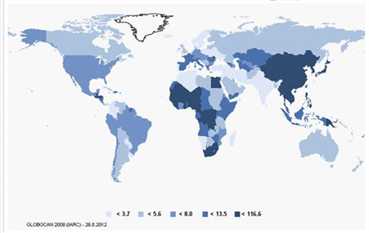
Incidence and Mortality of HCC Worldwide (per 100,000)

中国是HCC重灾区
超过百分之七十病例中,肝硬化晚期发展为HCC。风险因素:病毒性肝炎,酒精,黄曲霉素
统计中HBV是引起HCC的主要因素
In more than 70% of all cases, HCC develops in patients with advanced liver cirrhosis. In 90%, the responsible risk factor is known. The main risk factors for liver cirrhosis and HCC strongly depend on the geographic region. Worldwide, the most important risk factors are viral hepatitis, alcohol und aflatoxin exposure (Table 1). 54% of all HCC can be attributed to hepatitis B and 31% to hepatitis C. Interestingly, signs of advanced cirrhosis such as portal hypertension correlate with the development of HCC.
Distribution of Risk Factors by Geographic Region (adapted from EASL-EORTC Clinical Practice Guidelines 2012 [11])
四分之一慢性感染者最终发展为HCC
Up to 25% of all chronically infected individuals will eventually develop HCC
并非HCC发生在肝硬化患者,慢性HBV中,非肝硬化患者有百分之三十患者可发展为HCC。
HCC does not exclusively occur in cirrhotic livers, but also in non-cirrhotic livers of nearly 30% of high viremic patients.
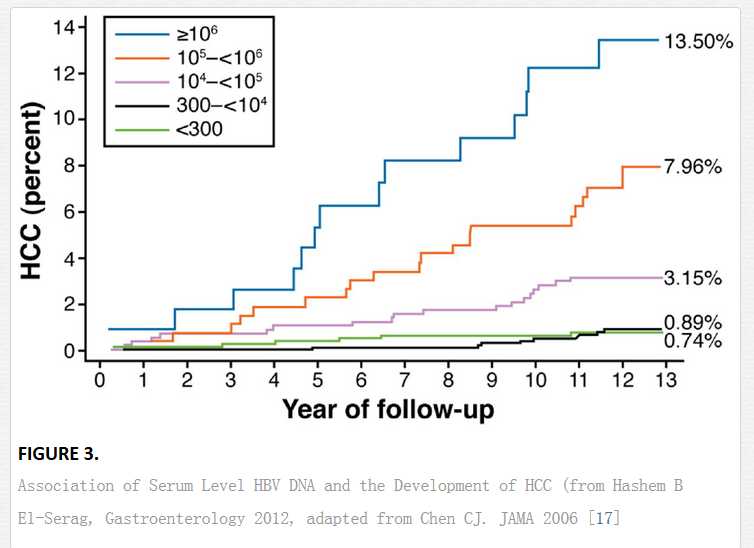
HCC风险因素:长期HBV DNA大于10的2次方,高转氨酶,HBV e抗原阳性,HBV C基因类型感染,男性,超过四十岁,家庭HCC历史,来自高发区的人口,HDV,HIV,HCV交叉感染,黄曲霉素和酒精的接触。
The risk for the development of HCC of HBV infected patients is elevated to 5 to 100fold. Main risk factors are long-term high viremia (>2000 IU/ml) (Figure 3), high aminotransferases, positive HBeAg and infection with HBV genotype C [15;16]. As patient related risk factors, male gender, more than 40 years of age, positive family history for HCC, migration background from hyperendemic areas, co-infection with hepatitis D virus, HIV or HCV and exposure to alcohol or aflatoxins were identified.
HBV如何诱导HCC的分子机制尚不明确。持续炎症和细胞损坏导致细胞最终破坏,导致遗传性改变积累。
The molecular mechanisms of hepatitis B virus-induced hepatocarcinogenesis are not completely understood. Ongoing inflammation and cell damage lead to an increase of cell turnover, which finally results in an accumulation of genetic alterations. These may also be caused by chromosomal integrations of HBV, which can be found in up to 80% of all HBV-related HCC. Furthermore, some viral proteins can transactivate growth factors and proto-oncogenes like c-MYC.
HBV治疗搜索关键字 HBV treat guideline (在WHO找)
Patients with chronic hepatitis B or hepatitis B/D co-infection should be treated according to current guidelines.
抑制病毒可以预防肝硬化,降低HCC概率
Sustained HBV suppression can prevent the progression to cirrhosis and hence lower the risk for HCC.
一旦肝硬化形成,核苷酸药物潜在预防能力大大降低。超声波和甲胎蛋白半年检查一次,可以预测HCC
Once cirrhosis is established, the preventive potential of antiviral drugs in chronic hepatitis B has not been robustly demonstrated. Ultrasound examination every six month +/- AFP measurement for HCC screening in patients at risk is strongly recommended.
HBV DNA 水平越高,HCC概率越高
HCV比HBV更容易诱导HCC,第一例HCV病例发现在日本,随后通过血液传播(输血,血液器具感染)
Similar to hepatitis B, patients with hepatitis C are at higher risk to develop HCC. Worldwide, over 180 million people are infected [2% of the global population) and about 30% of HCC are HCV-related.
In the late 1920s, the first HCV infections occurred in Japan. Not before the 1940s, it spread in Southern Europe and in the 1960s and 1970s many people in North America were infected, mainly due to intravenous drug use but also via medical procedures. The virus contaminated national blood supplies and circulated until the late 1980s. Nowadays, the highest prevalence of HCV is found in Egypt, being 9% countrywide and up to 50% in certain areas [18]. Recent data suggest that HCC occurs decades after infection and that the risk is strongly elevated in patients older than 65 years compared to younger patients [19]. Thus, the temporal distribution of the HCV-endemic is one reason for the differences in the incidence rates HCC in different areas.
HCV infection is chronic in most patients. It goes along with a variable degree of hepatic inflammation and results in cirrhosis in 10-40%. At the stage of cirrhosis, HCC is the main complication and the main cause of death. Compared to non-infected individuals, the risk for HCC is 17fold elevated. In contrast to HBV, in HCV infected patients, tumours occur primarily in the cirrhotic liver. The risk per year to develop HCC in patients with HCV-related cirrhosis is 5%. It increases when additional risk factors are present, e.g. genotype 1b, alcohol or cigarette consumption or a co-infection with HBV or HIV [20,21].
In contrast to HBV, HCV cannot integrate into the human genome. Instead, apparently several viral proteins have tumorigenic effects. In rodents, it has been shown that overexpression of NS3 induces HCC. Patients with HCV infection are recommended to obtain treatment according to current guidelines. Treatment options for hepatitis C are interferon alpha, ribavirin and more recently also protease inhibitors. In patients with sustained response, HCC incidence is markedly reduced [22]. Excepted to this protective effect are patients with evident cirrhosis. Thus, screening for HCC via ultrasound and eventually AFP measurement are recommended every six months.
过渡饮酒,香烟是提高HCC的催化剂
咖啡具有降低癌症的功效
Alcohol alone probably is not carcinogen. However, excessive alcohol intake is one of the most frequent reasons for liver cirrhosis and thus an important risk factor for HCC. Recent epidemiologic case control studies suggest that not only alcohol (in 10% of all HCC) but also tobacco consumption (in almost 50% of all HCC) is a relevant cofactor for hepatocarcinogenesis [23]. Particularly in patients with HCV, and to a lesser extent, with HBV infection, the risk to develop HCC increases significantly already with moderate alcohol and tobacco consumption [24,25]. A large retrospective study of 36,000 liver cancer related deaths in Chinese demonstrated a dose-dependent elevation of the risk to die of liver cancer in cigarette-smokers. Main risk factor in this population was HBV. While patients who smoked less than 20 cigarettes per day had a 32% increase of risk compared to nonsmokers, patients with a cigarette-consumption of 20 or more per day had a 50% increase of risk [26]. However, the study provided no information about simultaneous alcohol consumption. In contrast, numerous epidemiologic studies showed a protective effect of coffee on the development of liver cirrhosis and HCC [27]. To date, the underlying mechanisms are not yet understood
糖尿病,肥胖,BMI指数过高均可诱导HCC
糖尿病和高血压可以互相诱导
Prospective and retrospective studies identified diabetes mellitus as an important risk factor for the development of HCC, independent from the underlying liver disease [29,30]. Non-alcoholic liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH) are more and more regarded as a hepatic manifestation of the metabolic syndrome, which is characterized by the combination of obesity, insulin resistance or diabetes, dyslipidemia and arterial hypertension. In US and other western countries, NAFLD is the most common liver disease of adults. However, only 20% of the individuals with NAFLD present with steatohepatitis, while the majority only have steatosis. Isolated steatosis of the liver probably has no effect on liver-related mortality [31-33].
NAFLD is found in 75% of patients with diabetes and 90% of obese patients with a body mass index of more than 40kg/m2. Based on a cohort study of 900000 Americans, it has been proposed that men with a body mass index of 35kg/m2 or above have a 4.5 times higher risk for dying from liver cancer compared to men with a normal BMI. Similarly, a meta-analysis revealed a relative risk of liver cancer of 117% for overweight and 189% for obese persons [34]. The risk for developing HCC is less in NAFLD than in Hepatitis C but due to the increasing prevalence, NALFD and NASH are nowadays more often identified as underlying risk factor in patients with newly diagnosed HCC than HCV infection [35].
Currently, NAFLD is still believed to be underestimated as underlying risk factor for HCC. One reason is that once cirrhosis is established, key elements of NASH as hepatocellular lipid accumulation, ballooning injury and necroinflammation are no longer detectable in the cirrhotic liver [36]. Accordingly, the underlying disease in cryptogenic cirrhosis may be NAFLD in a considerable proportion of cases. Furthermore, NAFLD and other risk factors for HCC can occur simultaneously but mostly the second risk factor, e.g. HCV, is counted as the responsible risk factor. An alarming sign is that tumours develop in non-cirrhotic livers in up to 50%, meaning that the population at risk is higher than originally estimated [37].
Until now, neither a treatment for NAFLD or NASH, nor a strategy to prevent HCC in NAFLD has been established. A major focus certainly will be put on the insulin resistance of NAFLD patients. The results of several retrospective studies and meta-analyses suggest a preventive role of metformin in diabetic patients, while sulfonylurea drugs and insulin seem to facilitate the development of cirrhosis [38-40].
黄曲霉素在亚洲无处不在,并污染坚果,玉米,豆类,进入食物链。具有强烈肝毒素
One important risk factor for HCC is the exposure to aflatoxins in some geographic regions. The toxins of the fungus aspergillus flavus and aspergillus parasiticus are ubiquitous in parts of Africa and Asia. By contamination of corn, nuts and legumes they enter the food chain and affect the broad population. Aflatoxin by itself is biologically inactive and displays its full effect only after ingestion by activation to aflatoxin B1-8,9-epoxide. The electrophil epoxide binds covalently to DNA bases and thereby becomes mutagenic. Epidemiologic investigations revealed frequent mutations in the tumour suppressor p53 in these patients. Simultaneous exposition of aflatoxins and HBV infection results in a more than additive risk for HCC.
血色病和一类遗传性高酪胺酸血症 是遗传病,与HCC有关联。HCC有遗传易感性
In first place, hemochromatosis and hereditary tyrosinemia type 1 (HT1) are genetic diseases associated with HCC. Hemochromatosis is an autosomal recessive disorder due to a mutation in the HFE gene. It is characterized by an increased intestinal absorption of iron, resulting in an accumulation and deposition of iron in organs like liver, pancreas, skin, heart and pituitary. In the liver, progressive accumulation of iron leads to fibrosis and cirrhosis and promotes the development of HCC. Affected patients are at 20fold higher risk to develop HCC.
HT1 is an autosomal recessive inherited disease, which is characterized by progressive liver disease and damage of the proximal renal tubular cells. It is caused by a deficiency of the enzyme fumarylacetoacetate hypdrolase (FAH), resulting in an accumulation of the substrate fumarylacetoacetate (FAA). FAA causes oxidative damage and is mutagenic. Untreated, the lifespan is dramatically shortened. Patients die from acute or chronic liver failure or from HCC in the first two decades of life. Therapeutically, nitisinone (or NTBC), an inhibitor of the enzyme 4-OH phenylpyruvate dioxygenase (HPD) can prevent accumulation of FAA.
Beside disease-causing mutations, there is growing evidence for a genetic susceptibility for HCC. In line with this, the risk to develop HCC is higher in individuals with a family history of HCC [32]. A predisposing effect is being suggested for numerous single nucleotide polymorphisms (SNP). A relationship between the carriage of a SNP and HCC in the investigated cohorts was demonstrated for SNPs in various genes, for example HFE (rs1800562), UGT1A7 (rs17868323 and rs11692021), MDM2 (rs2279744), IL-1B (rs1143627), MnSOD (rs4880), TNFalpha (G-308), EGF (61*G, rs4444903), cyclin D1 (G870A) [41]. The common variant rs738409 C>G in the adiponutrin/patatin-like phospholipase-3 (PNPLA3) protein sequence has consistently shown to be associated with hepatic steatosis, advanced fibrosis and a higher incidence of cirrhosis in patients with alcoholic [42] and non alcoholic fatty liver disease [43] and chronic HCV infection [44]. In patients with alcohol induced cirrhosis it is a risk factor for the development of HCC [45]
总结:HCC风险因子:HBV,HCV,酒精黄曲霉素,影像学对于HCC早期检测非常有用
Worldwide, HCC incidence is increasing. The most important risk factors for HCC are hepatitis B and C, alcohol consumption and aflatoxin exposure. The increase of HCC in patients with steatohepatitis is alarming and is likely to be a major problem in developed countries in the future. Most HCC develop in cirrhotic livers but particularly in patients with hepatitis B or NASH, it can also occur in non-cirrhotic livers. Screening programs are important for all patients with liver cirrhosis to detect HCC in an early stage.
标签:
原文地址:http://www.cnblogs.com/biopy/p/5769619.html